- Visibility 39 Views
- Downloads 8 Downloads
- DOI 10.18231/j.ijor.2024.010
-
CrossMark

Operative management of chronic isolated rectus femoris rupture with semitendinosus graft and biofiber: A case report
Introduction
Rectus femoris tear is rare and often overlooked in emergency.[1] The majority of quadriceps muscle belly injuries can be successfully treated conservatively and for less active, older populations Non-operative management is reasonable.[2] The rectus femoris muscle, owing to its function across two joints and its composition of predominantly type II muscle fibers, is often prone to strains. These strains frequently manifest during activities that demand sudden, forceful movements, such as sprinting, explosive jumps, or rapid accelerations while running. Injuries to the rectus femoris are commonly seen during the initial acceleration phase of these activities. Additionally, forceful contractions, especially when met with resistance, can also result in strains. Initially perceived as minor, these strains can escalate to become limiting, particularly when an athlete is pushing physical boundaries. Sometimes, compensatory mechanisms can delay the recognition of the injury.[2] Common injury sites for the rectus femoris include avulsion ruptures from its origin at the anterior superior iliac spine or ruptures at the distal rectus femoris muscle (quadriceps tendon). However, substantial injuries to the muscle belly and musculotendinous junction occur less frequently and are typically treated conservatively.[2]
Interestingly, despite the various reported injuries and treatment approaches, there are currently very few documented cases in the existing literature describing the repair of an intrasubstance chronic tear of the rectus femoris muscle with a good outcome. This specific area remains unexplored within medical studies and clinical practices. Surgical treatment of rectus femoris tear seems to be a good option in Chronic tears. [1]
Case Reports
Patient information
A 19-year-old male presented to the orthopedic outpatient department 5 months following an injury sustained while running with complaints of pain and defect in the anterior aspect of the mid-thigh and was unable to continue running. The pain was associated with weakness of the quadriceps during hip flexion and knee extension. Medical, Family, and psychosocial history was not significant
Clinical findings and timeline
On examination atrophy of the quadriceps muscle was noted and a 2 cm palpable gap in the muscle bulk on extending the knee during quadriceps contraction. This was tender on palpation. Tenderness over the midthigh and palpable defect with Pain upon resisted hip flexion or extension were seen. Clinically the quadriceps power was reduced (3/5)and there was no neurological deficit.
The patient experienced sudden onset Sharp pain over the anterior aspect of the midthigh while running during a kabaddi match and eventually developed swelling and bruising 5 months before he came to OPD after which he underwent conservative management in the form of Rest, ice compression, and protected weight bearing and functional movement training with gentle strength training. But the Patient could not return to the pre-injury level of sports for which the patient came to us for further management.
Diagnostic assessment
Ultrasound and MRI imaging were done to confirm a complete intrasubstance tear of the rectus femoris muscle. The distal half of the left rectus femoris with retraction of its tendon was seen in the MRI

Therapeutic intervention
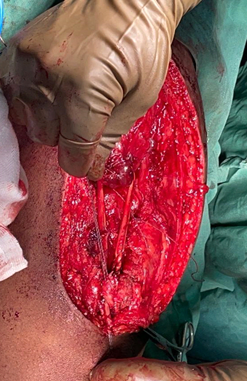
A vertical anterior incision over the defect was made, a fasciotomy done, and dissected from the quadriceps belly.
Intraoperatively, passive complete flexion was done to judge the exact length of the defect to fill the defect between the muscle belly and the Quadriceps tendon. A substantial 15 cm defect in the middle third of the muscle, accompanied by thinning and stretching of muscle fibers was noted. The defect was measured in flexion, extension, and midflexion optimally to avoid excessive tightness or laxity.
Initially, the surgeon attempted to address the issue by excising the scar tissue, freeing the muscle belly, refreshing the muscle ends, and performing a Kessler stitch. However, this primary repair technique was deemed inadequate for ensuring sufficient stability and support for early mobilization and functional recovery.
To fortify the repair, the muscular tunnel was made in a rectangular fashion in the Distal Rectus femoris belly. The tendon was secured to muscle in the tunnel. Semitendinosus graft was placed from the tip of the Rectus belly to the Distal Quadriceps tendon. The rip-stop technique was used with firewire to prevent cut-through or proximal migration of graft in muscle so that muscle won’t cut through or lose its desired position. A rigorous assessment of the repair's integrity throughout the knee's complete range of motion in flexion and extension was conducted before wound closure.
.

Follow-up and outcomes
In the postoperative phase, the patient underwent a systematic planned rehabilitation protocol. Initially, he was allowed full weight-bearing mobility while wearing a hinged knee brace that restricted movement from 0–30 degrees for six weeks. Passive flexion physiotherapy was administered to achieve up to 90 degrees of flexion without the brace. After six weeks, significant progress was observed as the patient could flex his knee to 100 degrees, ambulate short distances without crutches, and perform a straight leg raise without experiencing fatigue.
By the three-month mark following surgery, the patient displayed remarkable improvements. He could walk comfortably without assistance, showcasing a complete range of motion in the knee joint, and no discernible gap was palpable in the previously repaired muscle. Additionally, the patient could actively engage in squat exercises, indicating a substantial recovery of strength and function. He continued his physiotherapy regimen focused on quadriceps strengthening exercises, contributing further to his rehabilitation progress.
At the four-month mark postoperatively, the patient reported being entirely free from pain, exhibiting the capacity to walk extended distances comfortably, and resuming normal activities without hindrance. Notably, he regained robust quadriceps tone and there were no palpable gaps, was able to extend his left knee against resistance with contraction of the Rectus femoris tendon and tightness in it indicating successful muscle healing and restoration. Also, upon static contraction of the Quadriceps, contraction of the rectus belly and superior movement of the Patella could be seen. The palpable gap was not felt anymore and the tautness of the Rectus femoris tendon was noted. Consequently, the patient was given clearance to resume training and participation in competitive sports, including Kabaddi, and demonstrated a return to his pre-injury level of performance without any limitations or restrictions.
|
Scoring systems |
Immediate postop |
3 Monthly follow-up |
4 Monthly follow-up |
Out of |
|
IKDC Score |
19 |
69 |
84 |
87 |
|
Lysholm knee scoring scale |
17 |
83 |
95 |
100 |



Ethics statement
Written informed consent was obtained for the publication of that case report and accompanying images. We conducted this study in compliance with the principles of the Declaration of Helsinki. Written informed consent for publication of the research details and clinical images was obtained from the patient.
Discussion
The rectus femoris muscle, a key component of the quadriceps femoris group located in the anterior thigh compartment, is the most superficial and anterior among these muscles. [3], [4] Its straight head originates from the anterior superior iliac spine, while its reflected head seamlessly blends with the anterior hip joint capsule and the iliofemoral ligament, superior to the acetabulum. These two heads converge into a robust fascial aponeurosis, which then merges with the rectus femoris muscle tissue. [5] Functionally, it spans two joints and plays a pivotal role as both a hip flexor and a knee extender. Primarily, it facilitates knee extension, while also aiding in hip flexion alongside other hip flexors and ensuring pelvic stability during weight-bearing on the femur. Injuries to the rectus femoris muscle often involve a combination of eccentric and explosive muscle contractions.[6] These injuries, though infrequent, can manifest belatedly, emphasizing the need for maintaining clinical suspicion in patients experiencing chronic thigh pain following such mechanisms of injury. Notably, rectus femoris muscle belly injuries, distinct from the more common distal rectus femoris (quadriceps tendon) injuries, typically present with delayed symptoms, such as an anterior thigh mass and persistent pain. [6] Comparing the affected limb with the unaffected one often reveals noticeable asymmetry. When addressing these proximal muscle injuries, literature reviews reveal limited information. Notably, a sole report by Clare Taylor, Rathan Yarlagadda, and Jonathan Keenan discusses surgical repair for chronic ruptures at the proximal musculotendinous junction. [2] Biofiber, a system composed of synthetic industrial-strength polyester fibers, is designed to simulate the mechanical and anatomical properties of human ligament fibers.[7] These fibers are structured to resist fatigue, especially during flexion, and possess biocompatible properties for integration with human tissue. This integration fosters fibroblastic ingrowth, fortifying the overall repair structure.[8] While most quadriceps muscle belly injuries respond well to conservative management, even substantial tears in less active and older populations may warrant non-operative approaches. However, in cases like this young patient's, where five months of physiotherapy and non-operative management failed to yield the necessary functional recovery for resuming vigorous physical activities, operative intervention became imperative. Utilizing Biofiber and semitendinosus graft to reinforce by a Rip Stop technique facilitated immediate full passive knee flexion and extension. Coupled with an early graduated physiotherapy regimen, this approach enabled the patient to return to running and competitive sports at his prior level without any limitations.
Source of Funding
None.
Conflict of Interest
None.
References
- L Meller, MC Oca, K Wilson, M Allen, E Smitaman, S Kalavacherla. Intramuscular Degloving Injury of the Rectus Femoris From Kickball: A Case Report and Review. Cureus 2023. [Google Scholar] [Crossref]
- C Taylor, R Yarlagadda, J Keenan. Novel treatment (new drug/intervention; established drug/procedure in new situation): Repair of rectus femoris rupture with LARS ligament. BMJ Case Rep 2012. [Google Scholar] [Crossref]
- K Grob, T Ackland, M S Kuster, M Manestar, L Filgueira. A newly discovered muscle: The tensor of the vastus intermedius. Clin Anat 2016. [Google Scholar]
- T Fernández-Jaén, PG García. . Thigh/Muscle Injuries. InInjury and Health Risk Management in Sports: A Guide to Decision Making 2020. [Google Scholar]
- T Armstrong, B Pass, P Connor. The capsular head of the proximal rectus femoris muscle: a review of the imaging anatomy of proximal muscle injury in professional athletes - early experience. Br J Radiol 1136. [Google Scholar] [Crossref]
- JM Kary. Diagnosis and management of quadriceps strains and contusions. Curr Rev Musculoskelet Med 2010. [Google Scholar]
- MW King, J Chen, M Deshpande, T He, H Ramakrishna, Y Xie, E Jacob -Lopes, L Queiroz Zepka. Structural design, fabrication and evaluation of resorbable fiber-based tissue engineering scaffolds. Biotechnology and Bioengineering 2019. [Google Scholar] [Crossref]
- A M Blumenthal, T Bou-Akl, MD Rossi, B Wu, WP Ren, DC Markel. FiberWire vs FiberTape: Comparison of Bacterial Adherence in a Murine Air Pouch Wound Model. Orthop J Sports Med 2020. [Google Scholar] [Crossref]