- Visibility 11 Views
- Downloads 8 Downloads
- DOI 10.18231/j.ijor.2023.008
-
CrossMark

Total hip arthroplasty for neglected bed ridden case of ankylosing spondylitis - A case report
- Author Details:
-
Amit Ranjan Vidyarthi
-
 Sanjay Keshkar *
Sanjay Keshkar *
Introduction
Ankylosing spondylitis (AS) is a progressive chronic inflammatory autoimmune disease characterized by widespread spondylitis and sacroiliitis, mediated by CD8 T cells.[1], [2] The worldwide prevalence of AS is 1 to 1.4%[3] affecting males 3 times more than females[4] specially young adults (2nd to 3rd decade of life) with positive HLA-B-27.[5] It primarily appears as axial spondyloarthropathy affecting the sacroiliac joints and spine and hips. [6] The involvement of hips, knees and other peripheral / non-axial joints are though uncommon but frequently affected. [7] The hip is involved in 25% to 50% of AS patients and appears in its milder form as pain and swelling and slowly progressed to serious form as ankylosis and deformity if left untreated. [8] A severe hip deformity can seriously restrict the mobility of patient and affect quality of life of patients, and then the most viable option is total hip arthroplasty. [9], [10] We present such a case of Ankylosing spondylitis with a purpose to show that the severity can force a patient to become immobile (bed ridden) if left untreated and then there will be many challenges (related to THA and rehabilitation) to make them mobile and independent.
Case Report
A 31 year young male
Patient of Ankylosing spondylitis (with fixed Hips and stiffness of whole spine & knees) was brought to us in bed ridden condition with bed sores (Figure 1a). As per the history, he was suffering from this problem since last 4-5 years for which no special treatment received except for some symptomatic drugs for pain relief from local practitioners.
On examination
Bed ridden patient with bed sores on lower back with totally stiff spine. Both hips were ankylosed and had fixed flexion & abduction deformity. There was moderate flexion contracture of both knees also. Head & neck movements were negligible. In toto the whole body of the patient was stiff & immobile. He was unable to do his Activity of daily living (ADL) and dependent on others.
On lab test
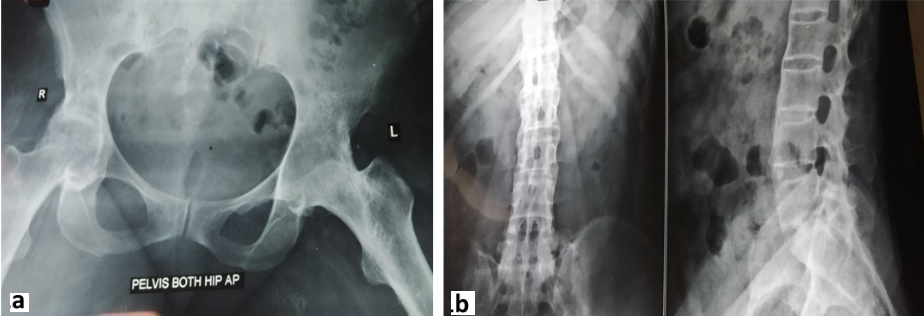
Patient was mildly anemic with elevated ESR and CRP. His HLA B27 was positive. Other lab tests were within normal limits. Radiograph of Pelvis with both hips showed complete bony ankylosis ([Figure 1]a). Radiograph of whole spine along with pelvis including both SI joint revealed complete fusion with typical Bamboo spine appearance ([Figure 1]b). The flexion deformities of knees are due to soft tissue contracture as there was no ankylosis radiologically. The history, lab test and clinico-radiological examination was more than sufficient to label the case as neglected bed ridden case of AS.
Decision making & treatment
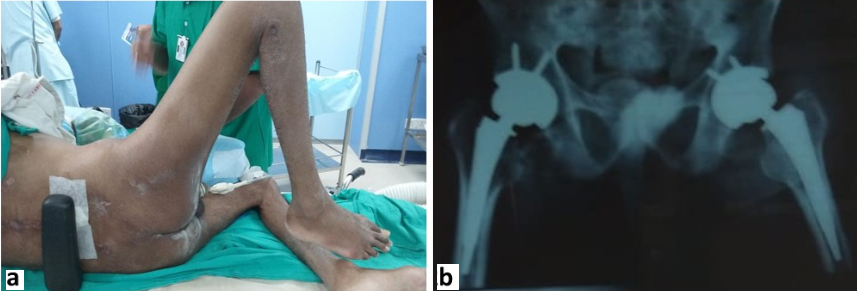
It was very challenging to manage but we took the challenge and started treatment. Family members were called upon to discuss the issues. Somehow, they convinced to take part in treatment process. Meticulous nursing care was provided to tackle his bed sores and stretching exercises for knees and feet contractures done. Then he underwent Uncemented total hip Arthroplasty (THA) of both hips (one by one in two different sittings). During first THA, soft tissue release (STR) for bilateral knee contractures were also done. Giving anaesthesia (Intubation) was also a challenge in such patient with completely stiff spine. But it was done successfully that too for twice by our anaesthetist. Pre-operative photograph ([Figure 2]a) of patient taken before surgery showing fixed flexion abduction deformity of hip with scars of bed sores. Post-operative radiograph ([Figure 2]b) was satisfactory.
Follow-up
Post-operative rehabilitation provided with help of our Occupational therapist & Physiotherapist. After about 3 weeks of 2nd THA, patient was able to stand and walk by walker and started doing his ADL by his own. After 1 month of 2nd THA, patient was discharged from hospital with advise to follow the rehabilitation protocol strictly. After 6 months of 2nd THA, patient had independent walking without support and able to do his ADL.
Discussion
THA is a viable option for fused hips of Ankylosing spondylitis (AS). These cases are very challenging right from its Preoperative evaluation. Degree of limb shortening, deformity, presence of a joint line, presence of greater trochanter and hip abductor function should be properly assessed before THA.[11], [12] Due to loss of ROM of hip, Surgical exposure and then dislocating the head of femur is difficult. In majority of the cases, one can dislocate the head by gradual rocking movement of hip but some cases may require An in-situ femoral neck osteotomy by angling the saw blade in line with native acetabulum and leaving sufficient quantity of bone in ilium [13] and then piecemeal removal of head with subsequent reaming to create acetabulum. While reaming, it is difficult to identify the true acetabular cavity and was done by triangulating the 3 vital surgical landmarks: the obturator foramen inferiorly, the sciatic notch posteriorly and the pubic bone anteriorly.[14] Femoral canal preparation is another problem in such cases because of abnormal proximal femoral anatomy with a sclerotic femoral canal and hence calcar split is common. One must be prepared to use modular implants to accommodate anatomical deficiencies or abnormalities. Adductor tightness is another issue for which percutaneous adductor tenotomy is required, if adductor angle is >30 degree.[15] Almost all such problems we faced in our case but managed nicely.
In conclusion, THA is key surgery for ankylosed hips in AS to make the patient mobile. By meticulous planning, management and rehabilitation, a bed ridden patient (like our case) will not only be able to stand and walk but also be able to do his ADL and become independent.
Conflicts of Interest
Authors declared no conflicts of interest.
Source of Funding
None.
References
- R Malhotra, G Sharma. Hip Replacement in Patients with Ankylosing Spondylitis. Orthop Muscul Syst 2014. [Google Scholar] [Crossref]
- E Lubrano, D Astorri, M Taddeo, A Salzmann, E Cesarano. Rehabilitation and surgical management of ankylosing spondylitis. Musculoskelet Surg 2013. [Google Scholar] [Crossref]
- J Braun, J Sieper. Ankylosing spondylitis. Lancet 2007. [Google Scholar] [Crossref]
- EN Kubiak, R Moskovich, TJ Errico, PE Di Cesare, . Orthopaedic management of ankylosing spondylitis. J Am Acad Orthop Surg 2005. [Google Scholar] [Crossref]
- LE Dean, GT Jones, AG Macdonald, C Downham, RD Sturrock. Global prevalence of ankylosing spondylitis. Rheumatology (Oxford) 2014. [Google Scholar] [Crossref]
- SM Goodman, M Figgie. Lower extremity arthroplasty in patients with inflammatory arthritis: preoperative and perioperative management. J Am Acad Orthop Surg 2013. [Google Scholar] [Crossref]
- R Cooksey, S Brophy, MJ Husain. The information needs of people living with ankylosing spondylitis: a questionnaire survey. BMC Musculoskelet Disord 2012. [Google Scholar] [Crossref]
- Y Ibn Yacoub, B Amine, A Laatiris. Gender and disease features in Moroccan patients with ankylosing spondylitis. Clin Rheumatol 2012. [Google Scholar] [Crossref]
- MM Ward, A Deodhar, EA Akl, J Ermann, LS Gensler, JA Smith. American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network 2015 Recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Care Res (Hoboken) 2016. [Google Scholar] [Crossref]
- G Kobelt, P Andlin-Sobocki, WP Maksymowych. Costs and quality of life of patients with ankylosing spondylitis in Canada. J Rheumatol 2006. [Google Scholar]
- HC Amstutz, DN Sakai. Total joint replacement for ankylosed hips. Indications, technique, and preliminary results. J Bone Joint Surg Am 1975. [Google Scholar]
- DJ Kilgus, HC Amstutz, MA Wolgin, FJ Dorey. Joint replacement for ankylosed hips. J Bone Joint Surg Am 1990. [Google Scholar]
- J Harkess, ST Canale. Arthroplasty of the hip. Campbell’s Operative Orthopaedics 2003. [Google Scholar]
- YH Kim, SH Oh, JS Kim, SH Lee. Total hip arthroplasty for the treatment of osseous ankylosed hips. Clin Orthop Relat Res 2003. [Google Scholar] [Crossref]
- AB Joshi, L Markovic, K Hardinge, JC Murphy. Conversion of a fused hip to total hip arthroplasty. J Bone Joint Surg Am 2002. [Google Scholar]